The Challenge
Indus Hospital, Pakistan's largest free healthcare network, serves 6 million people annually in a nation highly vulnerable to climate change and frequent floods. To support health needs during disasters and in remote areas, Indus Hospital needed a low-cost, safe, and portable ventilator.
The key design requirements were:
- Safe: Active lung pressure monitoring, emergency stop, and manual mode.
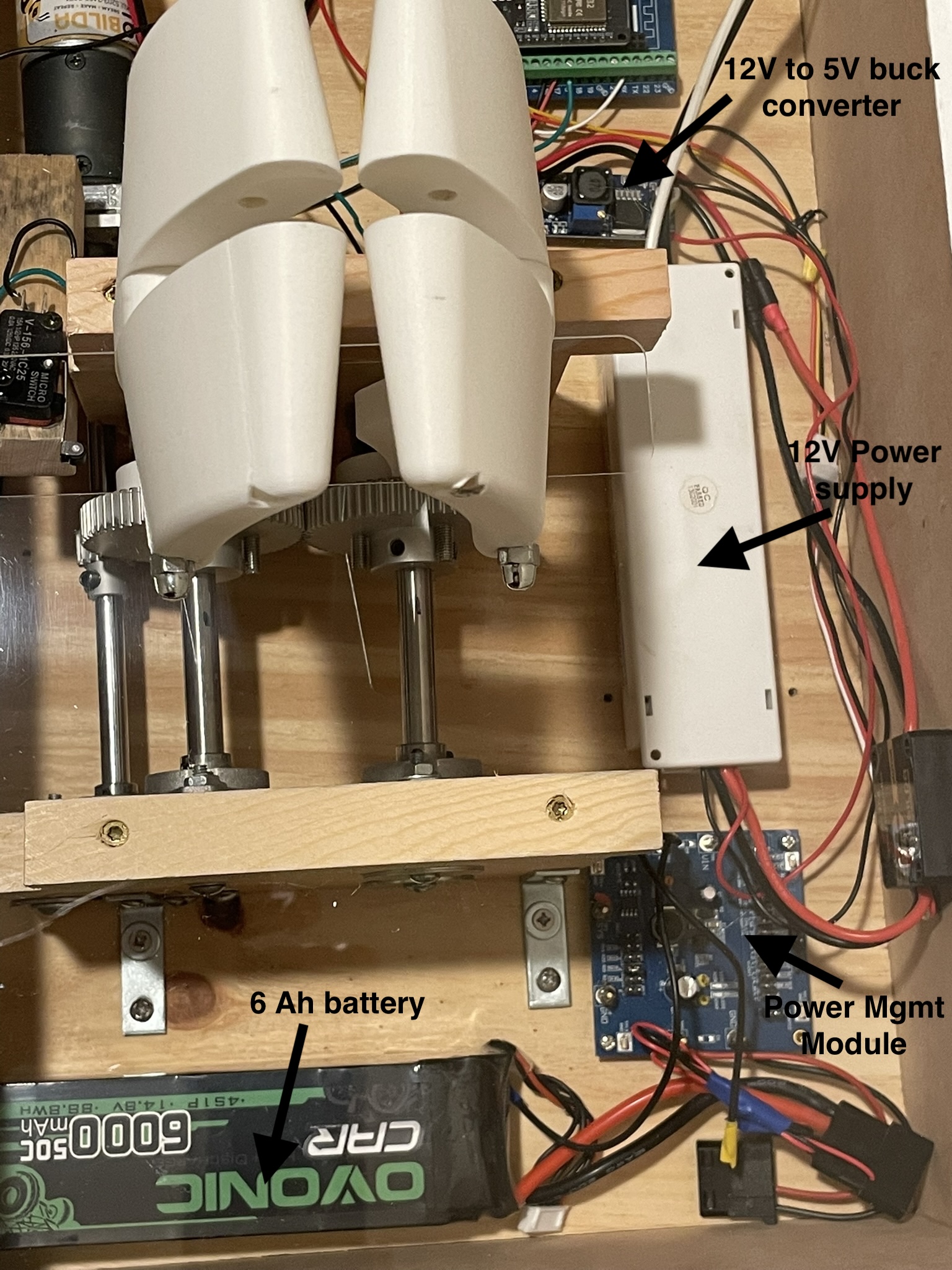
- Portable: Lightweight, compact, and 2+ hours of battery operation.
- Intuitive: Simple controls for BPM, Tidal Volume, I/E ratio, and alarms.
- Reliable: A simple, rugged design for field operation.
- Economical: Total cost of ownership under $1000 per device.
- Adult Use Only: (With child/infant support planned for future releases).